
In every market we follow at Northzone, there is usually some kind of major friction between suppliers and buyers that paves the way to create billion-dollar tech companies. However, the healthcare market in the US is a very special case, and not in a good way. Valued at ~$4trn, this industry charges its participants one third of its overall value in administration costs. This is staggering. In this market, consumers have little to no choice in the services they’re purchasing – they’re likely in urgent need and have no clarity on the costs they will incur. Some have to plan their entire life savings around these potentially devastating and often surprising healthcare expenditures. At the same time, the already undersupplied and overworked providers have to spend a huge portion of their revenues collecting the fees they are rightly owed.
This is the revenue cycle management process (RCM), which is currently how providers collect from payers such as Cigna, United, and Medicare. We believe there is a lot of room for improvement in this part of the healthcare value chain, and over the past six months, we’ve seen rounds into Adonis, Anterior (formerly Co:Helm), Cohere Health, and more. It’s not surprising that LLMs can create a step change in efficiencies, but more meaningful is the CFO/CIO interest and implementation of modern RCM tools. Some of the largest enterprise health organizations in the country are engaging with brand new startups to try and automate systems that process billions in claims per year. This makes us incredibly excited about the rate of change that we are about to see in healthcare IT.
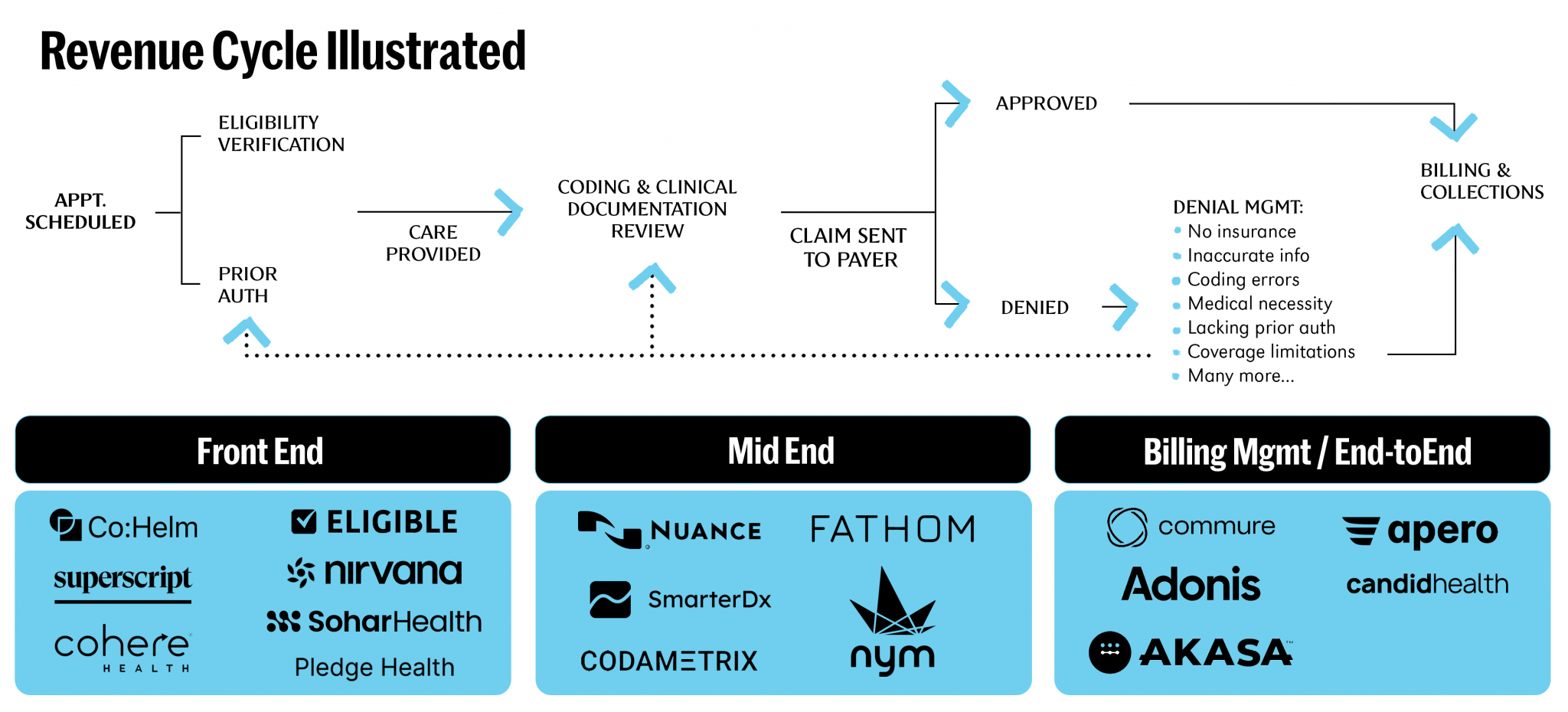
Delving deeper into the RCM opportunity: RCM is a complex process that starts with patient eligibility verification and pre-authorization at the front-end, extends to coding in the mid-end, and concludes with billing and claims management at the back-end.
While these processes are complex, expensive, and critical to revenue generation, it is still jaw-dropping to consider the sheer magnitude of spend that a system incurs purely on its revenue cycle. US hospital systems spend on average 8% of net patient revenue on revenue cycle management – a whopping $190bn+ annually. This spend is mostly incurred internally—staff salaries and clunky systems that allow administrators to liaise with insurance companies to get accurate prices and then charge and collect from patients.
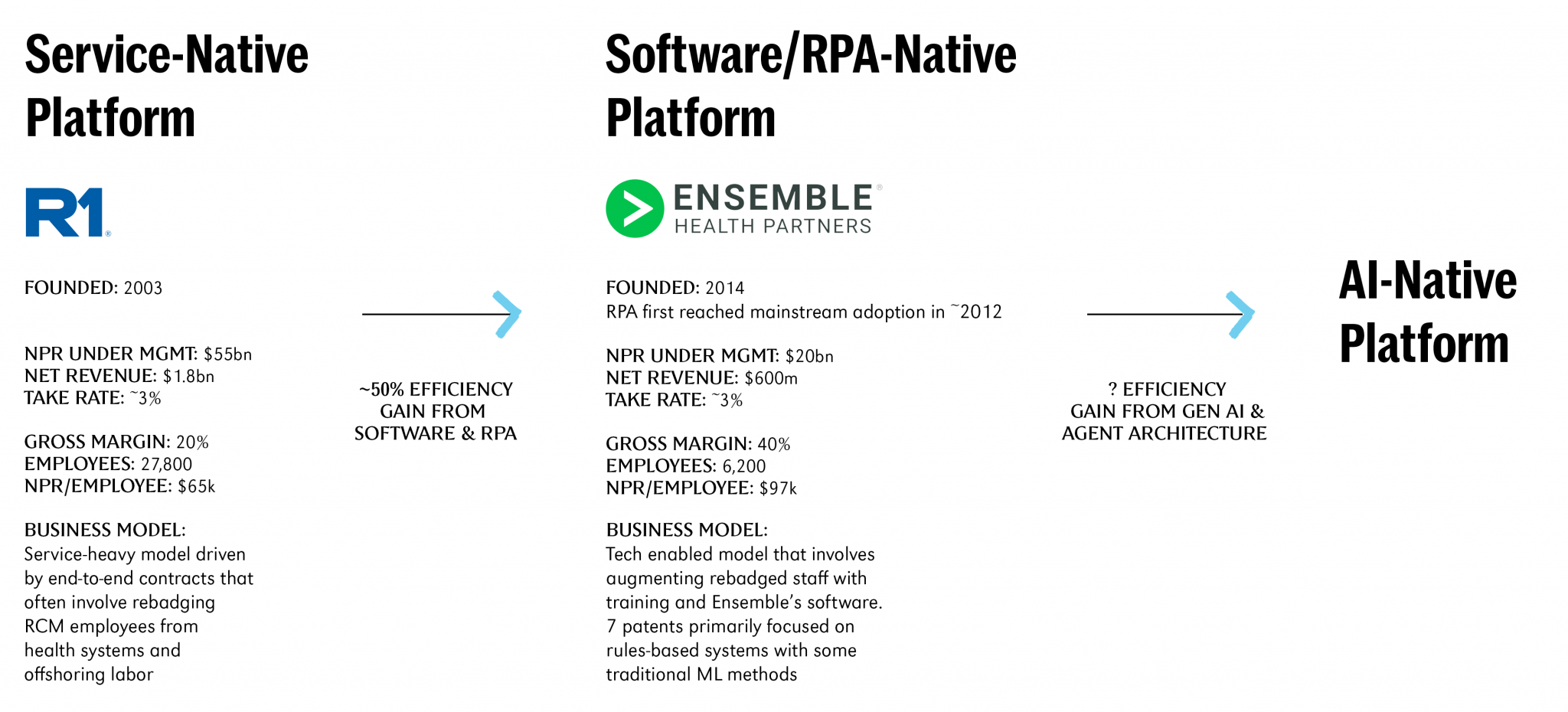
In the last decade, however, there has been a slow but clear trend towards outsourced end-to-end RCM players, who now own 20% of the market vs. 15% five to ten years ago. This has mostly been led by the first wave of RCM “tech” companies. R1 and Ensemble are the standouts, and they have promised some form of automated claims processing for a decade and deliver reasonably well, at 20% and 40% gross margins respectively. So what has changed?
Well, the AI hype cycle spares no industry. And in this case, AI has genuine potential to offer outsourced RCM with 1) high accuracy rates for customers and 2) high margins for the software companies.
Lots of start-ups are entering this space by starting with a specific wedge. There are scribing players like Abridge, Nabla, and Deepscribe, who may one day expand into coding and beyond. There are coding automation platforms like Nym and Smarterdx who think that addressing coding errors is the key to the RCM castle. And some start at the beginning of the cycle, focused on prior authorization and eligibility like Anterior (formerly Co:Helm), Nirvana, or Eligible.
While there are sizable opportunities in each segment, the next generational company to be built in healthcare will be a full-stack, tech + service platform that extends across clinical operations and RCM. There are three key reasons for this:
1. Billing management is, by definition, edge case management
Billing is a never-ending cat-and-mouse game between payers and providers. Insurance companies are constantly shifting reimbursement rates, benefits coverage, codes and documentation requirements, etc., creating a ton of edge cases that RPA & even traditional ML can’t scalably handle. This entropic dynamic is why 90% of human labor in RCM is spent on claims untouched by existing auto-adjudication systems.
2. LLM agents alone can’t solve this problem
There are many companies out there who are taking a software/AI-only approach to this problem. Don’t get us wrong, we do see the potential of building a suite of specialized agents fine-tuned by workflow, provider<>payer, specialty, etc. We also understand the fundraising appeal of a high-margin, software-only business model that can directly replace human billers. However, we think it’s important to be where the rubber meets the road.
The reality today is that standalone LLM agents aren’t up to par even for far less demanding workflows (e.g., CRM automation). We think that for the vast majority of providers, who deal with far higher stakes, adopting a pure AI solution will be a non-starter. Instead, we think the right approach is to build an AI-native platform with human billers who work alongside the software and AI tools/agents. In this business model, a core competency and competitive advantage is the process of perpetually understanding and applying the correct balance of human, software, and AI towards RCM.
We draw inspiration from history here. Ensemble Health built a software-enabled model that armed rebadged staff with Ensemble’s own software & RPA platform. They’ve been able to achieve 40% gross margins and $97k NPR/FTE, which represents a ~50% efficiency gain over legacy services businesses like R1. By leveraging LLMs we think an AI-native RCM platform will be yet another order(s) of magnitude more efficient and lucrative.
3. Unlocking true efficiency gains requires connecting clinical and admin silos
In addition to all of the above, an AI-native end-to-end platform has the potential to exponentially grow efficiency by the very nature of having integrated features to support clinical staff. An example best illustrates this:
Let’s say we learn that code ABC is now accepted by insurance more often than code XYZ for a given procedure. A normal biller would need to reach out to the physician, teach them the new requirements, and hope they remember the changes moving forward. Contrast that with an integrated system, which would be able to bake new documentation requirements directly into the note-taking interface, thus ensuring the physician creates the proper documentation every single time moving forward.
These types of unified experiences are what will ultimately move the needle in healthcare, rather than “just” building a business that makes existing labor pools more efficient.
If you’re building a wedge product, or already working on something end-to-end in RCM, we’d love to chat – Aaron, Molly


