
If you have been listening to any of the earnings calls recently for fast-food or snack food companies, you may have heard that CEO and CFOs are being quizzed about how Ozempic and Wegovy are affecting the health of their business. After being challenged about their AI strategies, they are now being put to the fire about whether their business will struggle if people consume fewer calories than before.
And it’s for a good reason: in the last year diabetes drugs and weight loss inhibitors (GLP-1) have added $100m to employee insurance costs to a large shipping company, lifted the economy of Denmark by becoming Europe’s largest market cap, and led to a pullback in spending on food at the world’s largest supermarket, Walmart.
While the impact of the GLP-1s is becoming well-understood in the public markets, fewer in the private markets are questioning how the proliferation of GLP-1s will affect their business model. At Northzone, we’re excited about the healthcare opportunities and have shared below our latest Perspective on the space.
Understanding GLP-1 Inhibitors’ Current and Future Landscape
In order to understand the impact of GLP-1s on VC-backed startups, it’s first helpful to set the level on what the state of play of GLP-1 inhibitors are today. Currently, only one (Wegovy) is covered to treat weight loss, with Ozempic, Mounjaro, and others covered by insurance to treat diabetes. While some people have been able to find receptive doctors who will give them a prescription, many pay out of pocket. The large sticker price of these drugs (~$1300 a month) is causing many insurance companies to pull back on their coverage due to skyrocketing costs. This in turn is causing an interesting calculus playing out between health insurance companies, self-insured employers, and consumers.

Obesity-related illnesses may be the number one driver of deaths in the world with cardiovascular diseases and therefore decreasing obesity has a clear ROI. Are those health benefits worth $1300 a month? $500 a month? Determining the strike price at which putting up barriers of entry is heavily dependent on how much confidence payers have that the effects of these drugs will last. We know that most people gain weight back when they get off the drugs, so payers may require some behavioural intervention to accompany drug intake.
While anyone who knows how the evolution of GLP-1s will play out, there are a few certainties:
- The drugs will get cheaper as more competition is introduced and a pill version becomes widely available
- Demand for GLP-1s will continue to increase exponentially as awareness of their effectiveness increases
- Coverage will increase as Wegovy and other GLP-1 inhibitors get approved for additional use cases such as cardiovascular health and addiction
- Finally, they are only going to get more effective. This all points to a world in which coverage expands and price decreases which will further supplement the demand and catapult GLP-1s further into the mainstream
With that in mind and for all that we can confidently predict, there is an equal amount of uncertainty and risk for how GLP-1 usage and coverage will evolve:
- While GLP-1s will decrease in price, do they remain elevated to the point that health insurance companies and self-insured employers are motivated to restrict access to them?
- How will coverage vary across different health insurance plans? If coverage is limited to large self-insured employers and isn’t covered by Medicaid or commercial plans, then there is a risk that there will be an inequitable distribution of these drugs, ruining their marketed fix to health disparities
- How will GLP-1s be used in conjunction with other behavioural health interventions? Given the novelty of these solutions, there is no learned and agreed-upon way to incorporate GLP-1s into a holistic weight-loss plan
- Are there any long-term side effects? While GLP-1s like Ozempic have been used since 2017 for diabetes, we have yet to see the effects of long-term usage of these drugs
Focusing On The Effects: The Broad Impact of GLP-1 Inhibitors
On People
What does a world in which 10-30% of Americans are taking GLP-1s look like? We ran a study with hundreds of people currently taking GLP-1s and found that:
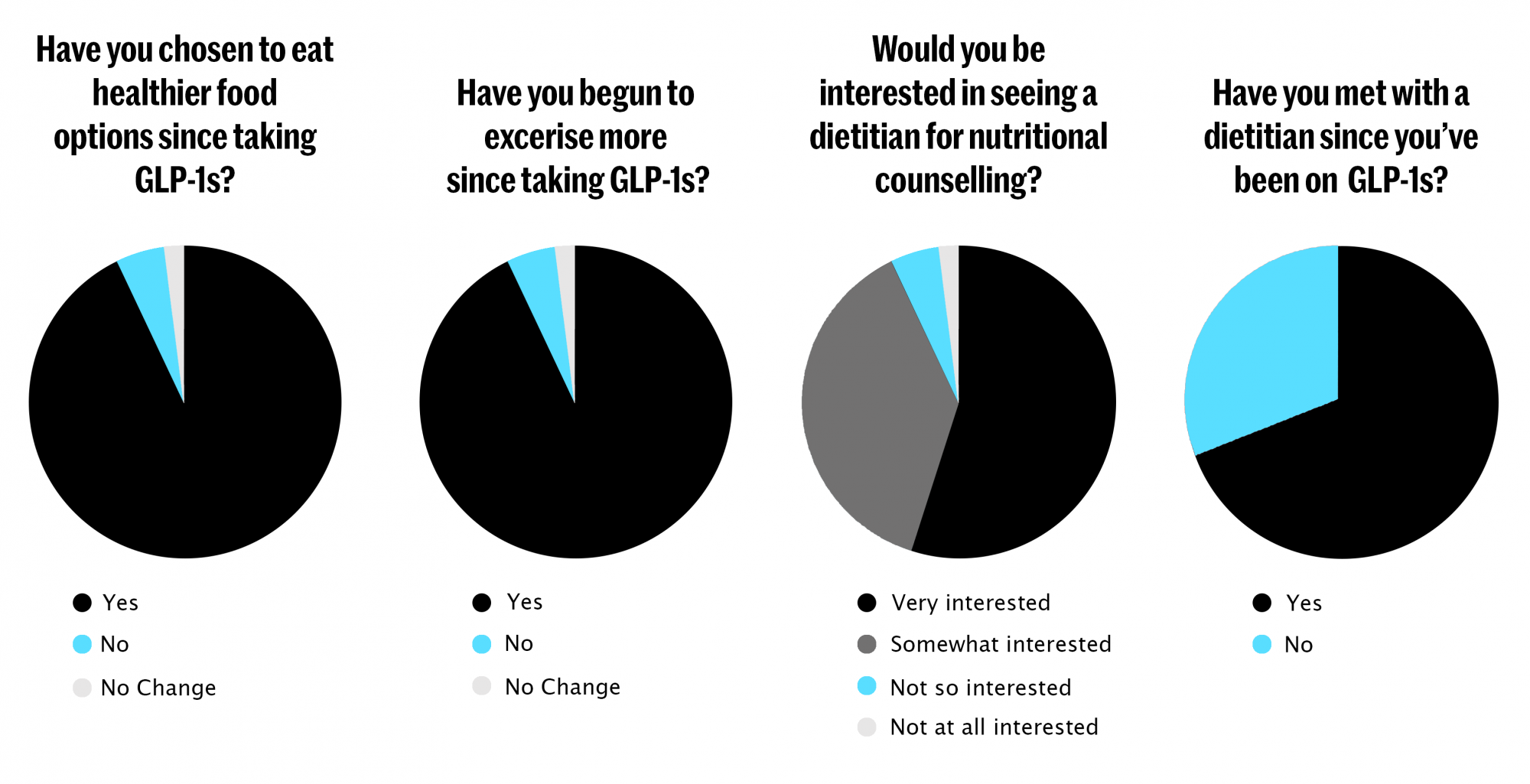
While many have speculated that due to the impressive effectiveness of the drugs, people would not be incentivized to exercise or eat healthier, our initial analysis suggests that the opposite is true. Once people started losing weight they felt more empowered to positively impact the rest of their lives. This tracks with what Charles Duhigg found when he wrote the Power of Habit, as“keystone habits” have a ripple effect with will influence the rest of our lives once integrated. Still, GLP-1s can often work too well, and many people suffer from malnutrition due to the extreme suppression of their appetite. That is why it is becoming more widely accepted to pair GLP-1 intake with consulting a dietitian or nutritionist to help balance out the lack of food consumption.
On Health Systems
In a world where people are regularly taking a GLP-1, our healthcare system looks very different. Less hospital visits, fewer obesity-related deaths, and more time spent on preventative care. While it is not widely understood how to incorporate GLP-1 inhibitors into longer-term healthcare plans today due to their novelty, best practices will begin to emerge and become incorporated into doctor’s care plans. In a perfect world, GLP-1s could help reduce the inequities in obesity and relieve underfunded healthcare systems of a great burden.
The role of Pharmacy Benefit Managers (PBMs) will be even more closely scrutinized. As employers and payers have looked to incorporate additional prior authorization guidelines that restrict who can get a GLP-1 prescription, we have heard of PBMs stepping in and threatening them with reduced rebates as PBMs are largely incentivized to encourage more prescriptions. Reducing prescription drug prices has been one of the few areas of bipartisan agreement and increased regulation of PBMs has often been cited as an area of agreement.
As obesity has become a large driver of serious illness, primary care physicians (PCPs) have become the frontline for helping people manage their weight. Nutrition and weight management are not what PCPs are best suited to handle, as can be evidenced by the food pyramids many PCPs give out at offices. If GLP-1s help reduce the number of people coming into PCPs with weight-related issues, PCPs will have more time to focus on the preventative care and triaging they were trained for.
WHERE TO INVEST: Navigating the Health-Tech Investment Landscape
But we are venture capitalists! So let’s get down into how all of this shakes out to affect different health-tech startups.
Directly Affected
- Obesity Management:
Startups in this space (Form Health, Wondr, Calibrate) are well-positioned to work with self-insured employers and even payers to help companies run their GLP-1 strategy. As we mentioned previously, companies don’t want to prescribe GLP-1s to everyone, but also want to make sure that the right people get it. These startups can act as a triaging layer that sits between patients and GLP-1 prescriptions or other weight-loss solutions. - Diet and Nutrition Platforms:
Diet becomes even more important when people take GLP-1s as maximizing the few calories that you consume for nutritional impact is paramount. Companies such as Berry Street, Nourish, and Fay Health will see tailwinds due to the increased demand for dietitians and ubiquitous healthcare coverage (68% of Americans are covered by insurance to see a dietitian a few times a year). - Digital Pharmacies
The positive effect here is pretty evident, as demand for GLP-1s increases, digital pharmacies like Thirty Madison and Hims will see increased volume for these products. Yet their inexperience with healthcare billing and the high sticker cost of these drugs may mute their overall impact.
Indirectly Affected
- Glucose Monitoring
Continuous glucose monitoring startups like Levels, January, and Nutrisense will become great ways for patients and doctors to track patients’ progress with their GLP-1 usage and make sure that they are not experiencing any adverse side effects.
- Sleep, Meditation, Mental Health
As mentioned previously, good habits tend to cascade. Platforms that help people get access to mental health treatments, meditate, and sleep better should see an increased bump in demand as consumers seek out additional ways to improve their overall health. Companies like Calm, Open, Spring Health and Hero Journey Club may see a second-order improvement to their business from GLP-1s.
- Wearables
If people are exercising more, then they may want to track their progress and get suggestions on how to constantly improve their well-being. Wearables such as Oura and WHOOP should be well-positioned to help people gather this data.
While AI may dominate many VCs’ discussions, we believe that GLP-1s will have almost an equal-sized impact in the near term on consumer behaviour. Not in recent memory has a new drug been so effective and experienced such rapid adoption.
It’s tantamount to understand the implications of this uptake as you evaluate companies in the health-tech space and beyond. If you are building in the space and getting a boost from GLP-1s, please reach out to nickb[@]northzone.com or michelle[@]northzone.com


